Why is being Black a problem? As a Black woman and a Black future pharmacist, I constantly surprise people. I talk like I have an education; I walk like I have a purpose; and I live like I have a right. Unfortunately, this is not true for many patients who look like me.
We’ve been demonized and ignored and treated as less than human. We are locked out of mainstream society- told to swim against the current and “better ourselves,” only to meet the dam of double standards. This is not a model for health. What we need are role models, such as Dr. Blaise Ndukwe of Kalamazoo, Michigan, to show Black patients that we, too, can wear white coats. “As the only black pharmacist employed with Gull Pointe Pharmacy at the time, I felt a duty from the first day I stepped into that pharmacy to advocate for black and brown patients. While I enjoyed my interactions with all of the patients I assisted, my interactions with black and brown patients, specifically, always felt more special. The way they looked at me, the way they spoke with me. There was always some level of respect and awe there. To be the only young, black, male pharmacist at that pharmacy and one of the only black pharmacists in the city of Kalamazoo, MI. That duty to represent weighed heavily on my shoulders and I fully embraced it. My most memorable encounter was with a black patient who had come through the drive-thru for his monthly refill. The cashiers noted him as a “problem patient” because he never “knew what medications he needed to pick up.” Instead, I saw him as someone who needed more devoted time from a pharmacist. I offered to sit down with him to review all of his medications and he accepted. A few days went by, and I never heard from him again. Then one day, he walked in unexpectedly and asked for me. Sitting down with him to review his medications was an opportunity for me to not only educate him, but for him to open up to me about his experiences at the pharmacy. He talked to me about the personal struggles he faced in his life as a black man and the things he does now to give back to his community. As I listened to him speak, I realized how important it was for him to finally see a pharmacist who looked like him. I realized just how important it was for him to finally see a pharmacist he could be unapologetically black with. Our conversation meant a lot to him, not just from an educational perspective, but also a personal one. He left the pharmacy that day knowing that he had an advocate, someone who would have his back when the other employees labeled him as “difficult” and “drug seeking.” He left that day knowing that he had an advocate who looked like him. He never let me forget just how much our interaction meant to him. Whenever he called he would ask to speak to me, and if I was unavailable, he would let the technician know to tell me how grateful he was for my help. We developed a friendly relationship, and sometimes he would show me pictures of his garden. I always enjoyed my interactions with him. Those moments truly made me feel as though I was fulfilling the duty I gave myself when I first stepped into Gull Pointe Pharmacy.” -Blaise Ndukwe, PharmD Introduction written by: Christian Brown, UNC Class of 2023; PharmAlliance Student
0 Comments
 February in America is Black History Month. In the annals of pharmacy history, there is precious little concerning Black pharmacists. Leo Butts of Wisconsin wrote the first scholarly work compiling the contributions of Black pharmacists in 1920. He chose the topic for his Degree of Graduate in Pharmacy thesis and was encouraged to pursue this work by his mentor, Nellie Wakeman, the first woman instructor at the University of Wisconsin School of Pharmacy (1). Still today, we see minorities supporting minorities to reach their full potential. Throughout his writing process, however, Butts expressed his disappointment that there was “scarcely a reference to the Negro in pharmacy” in the greatest pharmacy history library in the US (2).
In his thesis, Butts acknowledges a truth that characterizes the Black experience: “it is absolutely necessary for the colored druggists to give not only as good but better services than his white competitors, if he is to be even moderately successful (2).” His work predates the National Pharmaceutical Association by 27 years (3). The only national option for the 1400 Black pharmacists at the time was to join the physicians and dentists in the National Medical Association (2,3). Only in the American South were state organizations available, and their main focus was improving sanitation in Black neighborhoods. In only 16 pages, Butts recounts the most complete history of Black pharmacists to date. Five years later, another student pharmacist writes on the subject. Mozella E. Lewis, likewise, bemoans the lack of Black recognition, and seeks to fill the gaps: “Mention has not been made…because our people have been timid and no other people have thought enough of us to give us serious thought (4).” Even so, Lewis’s words are tainted with the Eurocentric disdain of her African roots as, after extolling the progress of Greeks and Hebrews, she complimentarily concedes that her ancestor, “in his savage way, was a great pharmacist.” Her thesis contains lists of names, cities, and achievements of Black pharmacists beginning with James T. Wormeley, the first graduate of the Pharmaceutical College of Howard University. He graduated in 1870 from the program started three years prior. Following the list of Howard graduates, Lewis lists Black graduates from White institutions, approximately 100 in total, along with their successes. She closes with this: These statistics give us an idea of what the Negro has done in pharmacy, and should encourage the young Negroes interested in this work to improve the many branches of this science in which the Negro has become famous and further develop those phases in which he seemingly has not yet entered to any great extent, so that the Negro will be an outstanding light in the development of pharmaceutical science (4). Written by: Christian Brown Bibliography 1. Bond G. Leo Butts, UW Pharmacy Pioneer . UW Madison School of Pharmacy Historical Alumni Information. https://pharmacy.wisc.edu/alumni-friends/events-awards-programs/historical-information/leo-butts-uw-pharmacy-pioneer/. Accessed January 13, 2021. 2. Butts LV. The Negro in Pharmacy. 1920. 3. NPhA - Home. https://nationalpharmaceuticalassociation.org/. Accessed January 14, 2021. 4. Lewis ME. History of the Negro Pharmacist. Am Drug. 1925. 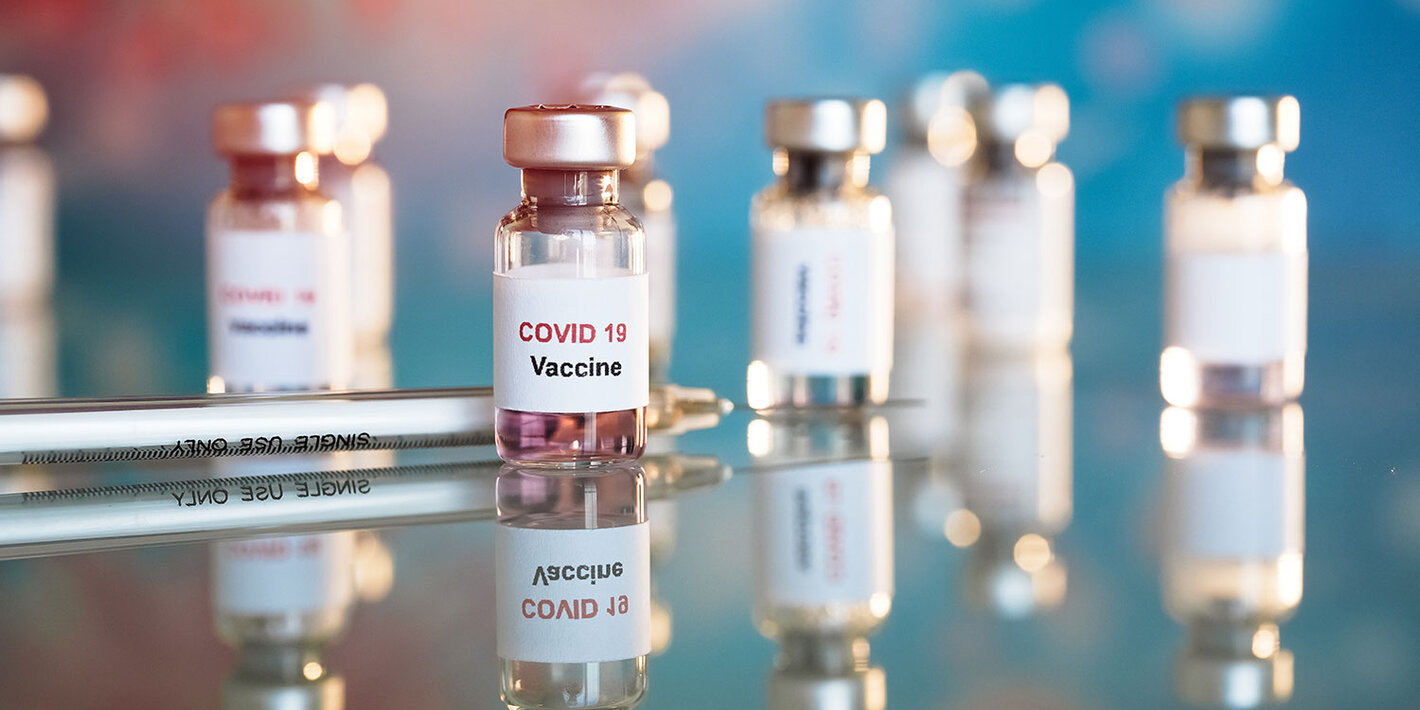 With roughly 71 million COVID-19 vaccine doses administered worldwide, 24.5 million doses given in the United States alone, humanity is experiencing one of the largest-scale global health efforts in history. There are dozens of different COVID-19 vaccines in various stages of development throughout the world that have the potential to be approved. As of writing this article, the World Health Organization (WHO) has identified 63 vaccine candidates in the clinical phase. Currently, the vaccines authorized for emergency use in the United States are the Pfizer-BioNTech and Moderna mRNA vaccines. These vaccines are a great first step into widespread vaccination, but there are several barriers limiting their use.
One of the biggest challenges for mRNA vaccines is their extremely strict storage requirements for stability, which are not unique to the Pfizer or Moderna formulations. The Pfizer vaccine is supplied as a frozen, 5-dose vial that is stored between -80ºC to -60ºC and has to be thawed and diluted prior to administration. After dilution, they have to be stored between 2ºC to 25ºC and used or discarded within 6 hours from the time of dilution. The Moderna vaccine also comes in multi-dose vials but has slightly less strict temperature requirements. They are stored frozen between -25ºC to -15ºC, but can be stored refrigerated between 2ºC to 8ºC up to 30 days prior to first use. Another limitation is that the Pfizer vaccine is recommended for people aged 16 years and older, while the Moderna vaccine is approved for people aged 18 years and older. If these mRNA vaccines have so many drawbacks, what other options will there be in the future? Despite the fact that the only COVID-19 vaccines currently available are mRNA vaccines, this vaccine type is actually relatively new and uncommon. To date, there are no other approved mRNA vaccines on the market. According to the WHO’s novel coronavirus vaccine landscape, only 7 of the 63 vaccines in development are RNA based. An additional 9 vaccines under development are DNA-based. In contrast, there are 20 protein subunit vaccines in clinical development. Another 16 vaccines in the viral vector class as either replicating or non-replicating varieties with or without additional antigen presenting cells are also identified. In the whole virus vaccine category, there are 9 inactivated virus vaccines and 1 live attenuated vaccine. The latest vaccine that has been approved in the UK is a viral vector vaccine developed by AstraZeneca and the University of Oxford. The vaccine has a reported efficacy of 90% and is stable for refrigeration. Their clinical trials, which involved over 11,000 people, found the vaccine’s 90% efficacy figure in those that received a low dose followed by a standard dose. Surprisingly, in participants that received two standard doses the efficacy of the vaccine was only 62.1%. One of the major benefits of the vaccine is its price of $4 per dose, much lower than the $20 of the other available vaccines. However, there have been problems with supply and pricing. The UK has ordered 100 million doses, Australia has ordered 53 million, and the EU has a contract with AstraZeneca to provide up to 400 million doses in total, around 80 million of which were due this quarter. Unfortunately, AstraZeneca reported on January 22 that they will only be able to deliver 31 million doses to the EU and supply chain issues likely affect their other agreements as well. The U.S. still has not approved the vaccine due to delays in clinical trials. Some other major viral vector vaccines production includes Jannsen/Johnson&Johnson’s vaccine, which also has an agreement for 400 million doses with the EU once its year-long clinical trial is finished. They launched their phase 3 trials in Latin America and the UK in fall of 2020. The Ganekaya Research institute in Russia is also developing a viral vector, called Sputnik V, that has just entered phase 3 trials. It has a reported effectiveness of 92% and can be stored at normal fridge temperatures. Another U.S. based biotech company, Novavax, has recently finalized an agreement with Canada to purchase 52 million doses and concluded talks with the EU for up to 200 million doses for their fridge-stable protein subunit vaccine. The French company Sanofi and England-based GSK also have a protein subunit vaccine that is stable at refrigerator temperatures and can even be stored at room temperature for a short amount of time. The EU has already confirmed the purchase of 300 million doses of their vaccine. Additionally, Sanofi has just finished settling an agreement to assist in producing 100 million doses of the Pfizer/BioNTech vaccine just hours before writing this article. Information on vaccines in development in China is more difficult to obtain, but Sinovac’s inactivated vaccine is currently approved for emergency use in China. The country currently has the second highest number of vaccines given in the world at 15 million in total. Other countries have already reached agreements with Sinovac, such as Turkey approving 10 million doses of the vaccine. The latest figures of its effectiveness put it at around 50.4%, making it an unlikely contender at its reportedly $60/dose price tag. Sinopharm, which is a state-run company, is also developing two inactivated vaccines of its own. Reports of its efficacy are a little inconsistent but hover around 80% effectiveness. Regardless, the United Arab Emirates has already approved the Sinopharm vaccine earlier this month. The vaccines mentioned in this article are nowhere near an exhaustive list of all the potential vaccines that may come out to protect against COVID-19, which is great news. As the effort to push for global immunity to the virus that turned the world on its head continues, it’s reassuring to know that several different options will eventually become available for the public in the coming years. More than likely, a set of gold-standard vaccines will be developed in the years to come that will join the likes of influenza on the list of regularly scheduled vaccinations. Written by: Kervin Novido References: ● https://www.gavi.org/vaccineswork/covid-19-vaccine-race ● https://www.gavi.org/vaccineswork/there-are-four-types-covid-19-vaccines-heres-how-they-work ● https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines ● https://www.bloomberg.com/graphics/covid-vaccine-tracker-global-distribution/ ● https://www.fda.gov/media/144245/download ● https://www.fda.gov/media/144637/download ● https://www.novavax.com/covid-19-coronavirus-vaccine-candidate-updates ● https://clinicaltrials.gov/ProvidedDocs/60/NCT03681860/Prot_SAP_000.pdf ● https://ourworldindata.org/covid-vaccinations ● https://pubmed.ncbi.nlm.nih.gov/33306989/ ● https://fortune.com/2021/01/25/astrazeneca-covid-vaccines-europe-deliveries-south-africa-price/ ● https://www.news.com.au/world/coronavirus/australia/doctors-in-australia-will-bulk-bill-covid19-vaccinations-making-it-free-for-members-of-the-community/news-story/1e7beed205791af4fd60f45cfc56fe93 ● https://www.bbc.com/news/world-europe-55822602 ● https://www.bbc.com/news/world-asia-china-55212787 ● https://www.fiercepharma.com/pharma/despite-pfizer-s-high-efficacy-expectations-other-covid-vaccines-may-have-a-logistics-edge#:~:text=Pfizer's%20vaccine%20must%20be%20kept,35.6%20and%2046.4%20degrees%20Fahrenheit. ● https://www.cnn.com/2021/01/27/europe/sanofi-vaccine-doses-intl/index.html  The time had finally come to start my final immersion at Duke University Hospital in Durham, NC. I was excited, but mostly nervous about what I would experience. This immersion would be like no other because we were facing the early stages of the COVID-19 pandemic. PPE was running low at most hospitals, screening was not being done enough around the country, and more people were becoming hospitalized due to COVID-19. I was worried for my own health, but I knew Duke had taken great measures and precautions for the safety of not only the patients, but healthcare workers as well.
On my first day arriving at Duke, I immediately saw signs for wearing masks on campus everywhere. At Duke everyone on campus even outside of the hospital were required to wear masks at all times. As soon as I entered the hospital my temperature was taken, I was asked questions regarding my symptoms, and was given a new sticker each day to wear to show that I was healthy. My first month of rotations was in cardiology. One concern in cardiology, was the resemblance of certain classic symptoms such as shortness of breath and cough for heart failure being similar to COVID-19. Fortunately, all patients were screened rapidly for COVID-19 when admitted, so the chances of these symptoms being COVID-19 were relatively low. Since I was doing my clinical direct patient care immersion, typically this would require rounding in patients’ rooms with the team to decide on diagnosis and treatment. However, with COVID-19 pharmacy students were not allowed to enter patient rooms, but we were able to still round with the team going door to door to make recommendations. I remember seeing some interesting patient cases such as a patient who was diagnosed with Takotsubo cardiomyopathy, otherwise known as broken-heart syndrome. This patient was a previously healthy female and had a normal ejection fraction until her husband unexpectedly passed away. Her ejection fraction in the hospital was around 20% and was immediately classified as a heart failure patient due to this syndrome. During my second month at Duke I rounded in the pediatric floor. I loved working with and seeing all the children. It was devastating to see children in the hospital, however their resiliency and braveness at such a young age inspired me. All of the children I met from afar had such a positive attitude no matter what their diagnosis or illness was, which was truly astonishing to me. Some unfortunate few cases we saw at the hospital, which was new to all of the medical providers was MIS-C in regards to COVID-19. MIS-C otherwise known as multisystem inflammatory syndrome in children is a rare complication that can occur in this case due to an exposure to COVID-19 and can cause different parts of the body to shut down if not treated properly. I was able to present this new syndrome to the pharmacists along with treatment options. Although my last immersion was not exactly how I expected it to be, I am prouder than ever to be a part of a healthcare team in a time like this when healthcare workers are vital in defeating this pandemic. My appreciation for all medical providers and frontline workers definitely heightened as they dealt with the most difficult challenges this pandemic offered. I hope to one day become a strong and resilient healthcare provider as they are. Written by: Sarah Mouna REFERENCE: https://www.dukehealth.org/hospitals/duke-university-hospital In the 1920s, Alexander Fleming’s discovery of penicillin kickstarted a whole new era of medicine. The impact was such that penicillin was used to treat pneumonia in soldiers on the battlefields during World War 2. And yet a century later in 2020, over 12,000 people die in the UK due to antibiotic resistance with the number increasing to over 700,000 worldwide. So how did antibiotics go from a “miracle drug” that could cure illnesses previously feared by physicians, to a source of concern for doctors worldwide? After the discovery of penicillin in 1928, infections which previously resulted in loss of life were now being adequately treated by antimicrobials. Antimicrobials include antibiotics, antivirals and antifungals. They are vital in preventing and treating infections. An infection arises when a pathogen enters your body and begins to multiply, with a pathogen being a microorganism (such as bacteria) that causes disease. Antimicrobial resistance occurs when microorganisms no longer respond to the antimicrobials designed to kill them. When antimicrobials lose efficacy as a result of antimicrobial resistance, people can succumb to any number of infections. It has become increasingly apparent that antimicrobial resistance poses a real threat to mankind. In fact, antimicrobial resistance has recently been reported by the World Health Organization (WHO) as one of their top 10 threats to global health. Antibiotics are an example of antimicrobials which are used very widely. They have applications in hospitals, community, food production and in veterinary production. The problem is that the more often antibiotics are taken, the less effective they are. This is because bacteria replicate very quickly- for example, E. coli undergoes mitosis every 20 minutes. During this process, mutations can occur. In general, the change is inconsequential but sometimes, the mutation can benefit the bacteria and give it characteristics that prevent it from being affected by an antibiotic. This trait is then favored via natural selection and the mutated strain quickly outnumbers the original strain. This means that when more people use antibiotics, different species of bacteria have a greater chance at developing these resistant traits. When doctors and GPs inappropriately prescribe patients with antibiotics for conditions like sore throat and sinusitis, it puts patients who genuinely need antibiotics at greater risk of harm. A study found that in general around 1 in 5 antibiotic prescriptions are issued inappropriately in the UK and considering how around 18 in 1000 inhabitants are prescribed antibiotics annually, one can imagine how great the number of people misusing antibiotics is. Antimicrobial resistance requires urgent attention. If action is not taken to combat this phenomenon, many modern medicines could become obsolete. Overcoming antibiotic resistance has been a priority for WHO since 2015. World Antimicrobial Awareness Week is an organized effort by WHO to increase awareness of antimicrobial resistance globally and to encourage practices among the general public, health workers and policy makers, which will prevent further emergence and spread of antimicrobial resistance. Antibiotic Guardian is another initiative that is being undertaken to slow the spread of antimicrobial resistance, specifically that of antibiotic resistance. It is a campaign that was launched by Public Health England in 2014 and aims to encourage health and social care professionals, students, educators in the human and animal health sector as well as members of the public to take action against the spread of antibiotic resistance. By pledging to become an Antibiotic Guardian, you choose to perform a simple action which protects antibiotics against the threat of antibiotic resistance. We can all do our part to stop antimicrobial resistance from spiraling out of control. Prescribers, such as doctors, should ensure that they are appropriately prescribing antibiotics and other antimicrobials, whilst patients should ensure that they take these medicines correctly and finish the full course of treatment. Good hygiene and infection control practices, particularly in healthcare settings, can also prevent infection and reduce the need for antibiotics in the first place. Immunization such as vaccinations are also very useful in preventing infections, further reducing the need for antimicrobials. These measures could reduce the use of antimicrobials and in turn, their misuse, such that we can avoid a future where people succumb to infections as they would have prior to the 1900s. Authors: Amelia Ryan and Nusayba Ali References:
 With all the technological advances of the modern age, it is reasonable that one might be led to think all drugs are developed through highly sophisticated, novel experimental methods and human ingenuity. There’s no way that a drug that cost millions of dollars to create could have come from a humble plant, right? In fact, of all the drugs approved from 1981 to 2014, only 27% were purely synthetic while 50% came from mimics, derivatives, or unaltered forms of natural products!1 There may be an air of exoticness or crudeness associated with natural products, but they are clearly prevalent even among the cutting-edge science of today and continue to occupy a significant space in medicine.
Two fields within the wide scope of pharmacy concerning natural products include pharmacognosy and ethnopharmacology. Pharmacognosy is the study of the biochemical and biological properties of drugs of natural origin as well as the search for new drugs from natural sources.2 Closely related, ethnopharmacology deals with the observation and experimental investigation of the biological activities of plant and animal substances used in the traditional medicine of past and present cultures of different indigenous groups.3 While one is in the realm of natural science and the other sits at the intersection of natural and social sciences respectively, the two are not mutually exclusive and both possess an acute understanding and appreciation of nature as a master chemist of diverse, complex molecules that provides invaluable resources for drug development. From drugs that can treat cancer to medicines that help relieve a simple headache, the range of drugs that have been created from the trees and microorganisms that make up the background of our lives is astounding. A compound first isolated from the purple-pink flowers of the foxglove plant has been used for hundreds of years to treat a condition first referred to as “dropsy.”5 Although the name for the condition of fluid retention in the heart and lungs has become more refined under the category of heart failure, the same active ingredient in those dried, powdered leaves has been used for hundreds of years and even now is sold and dosed as the familiar digoxin.4 Scientists continue to isolate and discover viable structures from natural products as they have done for centuries past, but now they have the technology and innovations of today to help guide them in not only creating new drugs but also understanding current drugs. The therapeutic windows for dosing, toxicity, and other factors are becoming better elucidated as we are able to narrow down optimal doses and even generate synthetic antibody-type antidotes to drugs such as digoxin. On the other hand, researchers at universities are exploring novel compounds from natural sources in treating disease states. For example, the universal yet poorly understood state of pain is currently being treated mostly with opioids, another class of drugs isolated from the opium plant. Researchers at the Boston Children Hospital have found a potential delivery system for TTX, a neurotoxin found in pufferfish.6 This treatment could potentially reduce dependence on opioids and dosing frequency and combat the opioid epidemic plaguing the world. However, the transition from traditional to modern society is not always so innocuous. The Matses people of Brazil and Peru remain isolated in one of the most carbon-rich, densest parts of the Amazon rainforest. As they are integrated into the outside world, the elderly medicinal shamans have found their knowledge at risk of being lost forever and have thus created an encyclopedic trove of information regarding their interpretations of disease states and various natural treatments, drawn from their environment in the rainforest.7 It is critical to preserve these wealths of knowledge passed down through generations of indigenous groups as they are disappearing at an alarming rate. As pharmacists, we have to keep in mind the important role traditional medicine continues to play in the lives of many patients who come from different cultural backgrounds. The advancement of modern medicine provides life-saving therapies for millions around the world, but we also cannot forget the vast influences traditional medicine exerts. What connects the two together is the limitless opportunities that natural products offered in the past, continue to offer in the present, and, undoubtedly, will offer in the ages to come. Authors: Aimee Ho and Anna Li 1. Newman DJ, Cragg GM. Natural Products as Sources of New Drugs from 1981 to 2014.JournalofNaturalProducts.2016;79(3):629-661. doi:10.1021/acs.jnatprod.5b01055. 2. AbouttheASP.TheAmericanSocietyofPharmacognosy.https://www.pharmacognosy.us/ what-is-pharmacognosy/. Accessed February 20, 2020. 3. Journal of Ethnopharmacology. Aims & scope - Journal of Ethnopharmacology | ScienceDirect.com.https://www.sciencedirect.com/journal/journal-of-ethnopharmacology/about/aims-and-scope. Accessed February 20, 2020. 4. Digitalis.https://www.ch.ic.ac.uk/vchemlib/mim/bristol/digitalis/digitalis_text.htm. Accessed February 20, 2020. 5. McLachlan A, McLachlan A. Weekly Dose: Digoxin, the heart medicine that may have givenusVanGogh'sStarryNight.TheConversation. http://theconversation.com/weekly-dose-digoxin-the-heart-medicine-that-may-have-given-us-van-goghs-starry-night-57980. Published August 23, 2019. Accessed February 20, 2020. 6. Liu A. Could a pufferfish toxin be a safe alternative to opioids? FierceBiotech. https://www.fiercebiotech.com/research/could-a-pufferfish-toxin-be-a-safer-painkiller-than-opioid. Published June 12, 2019. Accessed February 23, 2020. 7. Amazon tribe creates 500-page traditional medicine encyclopedia. Mongabay Environmental News. https://news.mongabay.com/2015/06/amazon-tribe-creates-500-page-traditional-medicine-encyclopedia/. Published December 20, 2018. Accessed February 23, 2020.  Happy New Year Everyone! As we celebrate, it is easy to forget that we are still in the middle of flu season! In the United States, flu season starts in October and continues through February. Last February, the state of North Carolina reported, through North Carolina Department of Health and Human Services (NCDHHS), at least 35 deaths from the flu. Many cases go undiagnosed or unreported, so it is likely that the actual number is higher. While the strain of flu is slightly different each year, getting vaccinated is always important to prevent catching and spreading the common sickness. According to the Center for Disease Control, the strain for the flu shot has changed recently.1 The changes are as follows:
Kansas and Brisbane are the locations that the strains were discovered for the 2019-2020 flu season and are predicted to be prevalent. The flu is always mutating, so this prediction may or may not work. Even still, the flu shot usually grants at least some form of protection and is recommended each year. Pharmacists have a major role in vaccinating communities against the flu. Starting in October 2019, North Carolina law allowed pharmacists to administer the flu vaccine to patients 10 years of age and older without a prescription. The new law also allows pharmacists to vaccinate patients from ages 6 to 10 years old with a doctor’s prescription.2,3 Prior to this legislation, patients had to be at least 14 years old to get their flu vaccine at a pharmacy. Furthermore, pharmacists are now allowed to give the HPV and hepatitis A vaccine to adults. This increases the impact that pharmacists can have on increasing vaccination rates in local communities. Staying current with all vaccinations is especially important as more and more individuals are choosing to forgo immunizations. In 2019, the CDC reported that only 75.2% of patients 24 months old received all seven recommended vaccines (MMR, DTaP, Hep B, 2 doses of Hep A, rotavirus, and influenza).4 Downward trends in vaccination rates have prompted some practices to take action. Blue Ridge Pediatric & Adolescent Medicine in Boone, North Carolina, implemented a “no shots, no service” policy and will not treat patients if they are not vaccinated for non-medical reasons.5 While this may seem harsh, the overall goal is to protect other patients and their families from potential disease exposure. It is important to remember that vaccinations both protect individuals and contribute to the immunity of the whole community. While students at UNC have been trained on vaccination techniques, laws, and other practices in North Carolina and the United States, students have to take an elective course for international vaccinations for travel purposes. In addition, students don’t really learn much about international vaccination laws and practices. Students should take a chance to research these topics if they can! As previously mentioned, many providers are refusing to take patients who have not received their vaccinations. In Australia, this becomes more of a government and legal issue with legislations titled No Jab, No Pay and No Jab, No Play.6 Both were enacted in 2016 to combat increasing outbreaks of preventable diseases and vaccination misinformation concurrently. Basically, the former legislation says that a child must be fully immunized for parents to receive certain tax benefits. The latter says that a child must be immunized to attend childcare in certain areas. According to the National Centre for Immunisation Research and Surveillance (NCIRS), exemptions do apply but objection is not a valid exemption. Visit the NCIRS website to learn more. There have been many vaccine myths and bits of misinformation spread by anti vaxxers and health-illiterate persons in the last few decades, some of which involve the US versus international immunization schedules. The most common is that the US gives much more vaccines than any other developed country.7 After taking a look at the vaccination schedules of other countries, one can find out that this myth is either false or exaggerated. While many European countries do not give as many vaccines overall, they do give more vaccines at an earlier age - this includes two doses of MMR and the chicken pox vaccine by the time a child is 15 to 24 months old. Some countries even give vaccines that the US does not give, such as the BCG and MenC vaccines. Another myth is that Japan banned the HPV shot. If a parent refuses the HPV shot for their child on the basis of this myth and its potential harmfulness, let them know that the HPV shot is still widely available in Japan - it is simply not actively recommended. All in all, the schedules are very similar between the US and other countries. It is important for pharmacy students to be aware of changes in immunization policy. From the local to national, and even on the international scale, legislation is always being updated to reflect the latest science and societal needs. As pharmacists, we have the ability to immunize patients and play a major role in preserving the public health of our communities. Even as students, we can volunteer in flu shot clinics and educate the patient population about current legal changes and the importance of vaccinations. Be sure to keep up with local laws and engage with the community to see the positive change that you can make. Authors: Linda Allworth and Zane Colon 1. APhA. New NC law lowers age for pharmacy influenza immunization, expands vaccines foradults.https://www.pharmacist.com/article/new-nc-law-lowers-age-pharmacy-influenza-immunization-expands-vaccines-adults. Accessed January 22, 2020. 2. Brown EA. New NC law lowers age for pharmacy flu shots, expands vaccines for adults. Asheville Citizen Times. https://www.citizen-times.com/story/news/local/2019/06/04/nc-law-lowers-age-pharmacy-flu-shots-expands-vaccines-adults-hepatitis-a-hpv/1337142001/. Published June 4, 2019. Accessed January 22, 2020. 3. CDC. Influenza (Flu). https://www.cdc.gov/flu/season/faq-flu-season-2019-2020.htm. Accessed January 22, 2020. 4. Immunization Schedules from Other Countries. Vaxopedia. https://vaxopedia.org/2017/04/23/immunization-schedules-from-other-countries/. Accessed January 22, 2020. 5. NCIRS. No Jab No Play, No Jab No Pay. http://www.ncirs.org.au/public/no-jab-no-play-no-jab-no-pay. Accessed January 26, 2020. 6. Ovaska S. No shots, no service: Pediatricians take tough stands while vaccination rates for young children in N.C. drop. North Carolina Health News. https://www.northcarolinahealthnews.org/2019/05/07/no-shots-no-service-pediatricians-take-tough-stands-while-vaccination-rates-for-young-children-in-n-c-drop/.Accessed January 26, 2020. 7. SUPPLEMENTARY TABLE 3. Estimated vaccination coverage with selected individual vaccines and a combined vaccine series* by age 24 months† among children born 2015-2016,§ by U.S. Department of Health and Human Services (HHS) region, state, selected local area, and territory – National Immunization Survey-Child 2016-2018, United States. 68.  The new year is the time everyone commits to a change for the future. From personal health goals to restructuring institutions, the world moves to become more efficient through innovation and optimization. Problems in healthcare continue to be an issue of how to effectively connect providers, patients, and payers, but integrating technology into the healthcare equation is creating an opportunity to meet those challenges. Pharmacy is a key place for it to happen. It is no secret that there are major companies worldwide creating new ways to deliver medication. Healthcare tech firm MedAvail have begun rolling out self-service kiosks capable of dispensing a prescription in under 90 seconds. Meanwhile, pharmaceutical giant Walgreens have begun testing drone delivery of medication. Pharmacy automation forecasting projects that revenue will grow 11% each year reaching $17 billion by 2023. In these cases, delivery is supervised by a licensed pharmacist that reviews medical history and offers patient counseling. These models are said to increase adherence and outcomes due to increased efficiency and care at the patient’s convenience. At the same time, other major companies are also investing in automation to stay relevant with competition. Scott Seidelmann, Chief Commercial Officer of Omnicell, a company that specializes in pharmacy automation, says, “It’s only a matter of time before people get their prescriptions from Amazon, but the impact that pharmacy has on the overall patient episode and its ability to influence not only patient care but economics across the continuum is driving the need for more automation.” Telepharmacy is also a growing field impacting rural chains and medium-sized health systems. It is currently predicted to be worth $22 billion in 2020, with the U.S. holding 13% of the market. Telepharmacy has improved to the point that pharmacists remotely can now do many of the things in-house pharmacists can do which allows in-house pharmacists to focus on other healthcare initiatives improving the efficiency of the health system. Some startup companies have even launched Discharge Management Programs this year to handle patient transitions from hospital to home or hospice. Numerous patients often fail to stay adherent, and money subsequently is lost due to readmission. By connecting patients and providers with a pharmacist anytime and anywhere, patient safety and efficacy is once again improved, and time and money can also be saved. A major addition to the digital health market is machine learning. IBM’s Watson Health is a division of IBM that facilitates clinical research and health care solutions through analytics, cloud computing, and artificial intelligence. Currently, Watson Health is working on being integrated into telehealth via a wearable device to monitor disease activity, health records, drug interactions, and even disease diagnosis at an accuracy level higher than a human. The shift from volume-based healthcare to a value-based care model has led to other shifts impacting pharmacy. There is room for pharmacists of today and tomorrow to incorporate technology to improve outcomes and expand their current role. Interesting to note, major companies are hiring “innovation consultants” that have pharmacy or medical backgrounds to come up with ways to make the “machine” run more smoothly. As we begin the new decade, pharmacists should be aware of how technology affects healthcare. It is also an exciting time, however, because the market is changing globally, and there is a growing need for pharmacists to be at the head of this change. Author: Mori Crocker  Some of our UNC student pharmacists celebrating American Pharmacists Month Some of our UNC student pharmacists celebrating American Pharmacists Month The role of a pharmacist is a unique one in the healthcare system. A pharmacist is the most well-informed health care professional on prescription and over-the-counter medications and is regarded by both patients and others in the healthcare field as a medication expert. The American Pharmacists Association (APhA), which is the largest association of pharmacists in the United States, named October as American Pharmacists Month to recognize the profession and their contributions to healthcare. This year, the slogan was Easy to Reach, Ready to Help. The goal was to let the public know that pharmacists are a readily accessible resource for them and that a simple conversation with the pharmacist can make a difference in their medication management. Pharmacists should take this chance to show patients the wide range of knowledge they have on not only drugs but also diabetes, high blood pressure, cholesterol management, and much more. There were various days to recognize the many team members in the pharmacy throughout the month. To kick it off, October 1st was APhM selfie day where pharmacists and their teams were encouraged to post selfies and pictures of their team with #APhMSelfieDay on their social media. Pharmacists were also encouraged to use #APhM2019 for any celebratory posts on social media during the month. National Women Pharmacist Day was on October 12th which was followed by Pharmacy Technicians Day on October 15th. At pharmacistmonth.com, APhA provided lists of activities that pharmacies could do as well as promotional items to use in their work space. Mayor Mark Kleinschmidt and Governor Pat McCrory declared October as American Pharmacists Month in Chapel Hill and the state of North Carolina back in October 2014. For this year, the sixth American Pharmacist Month happened with many activities in the Eshelman School of Pharmacy. According to Megan Byrne, a second-year PharmD candidate, the Carolina Association of Pharmacy Students (CAPS) led a series of activities to advocate the profession of pharmacy. They kicked off the celebration on the first day of the month with a tasty cake for all our staff and students in the pharmacy school. Later on, they got a photo booth on Family Day which is an annual event to introduce the profession to our students’ families. They also organized events to let student pharmacists talk with patients about our profession in an independent pharmacy. A feature on this was published in UNC’s student newspaper, the Daily Tar Heel! For more information, you can also read “Keeping the Dream Alive” which is an article about pharmacy identity and pharmacy history written by second-year pharmacy student Emily Meggs in celebration of American Pharmacists Month. Hopefully, we can expand these activities to other schools, communities, and hospitals in Chapel Hill in subsequent years to let more people around us be aware of the impact and value of pharmacists. We would also like to take this chance to thank everyone, every pharmacist, every pharmacy staff, and every student pharmacist, who do their best to promote change in our profession. Authors: Feiyun Ma and Allison Tsay
|


